Follow Us
-
+1 700 888 1234
-
Effingerstrasse 40 3008 Bern Switzerland



+1 700 888 1234
Effingerstrasse 40 3008 Bern Switzerland


 Lung cancer is a disease of the lung cells. As in other kinds of cancer, lung cancer cells grow and divide abnormally.
Lung cancer is a disease of the lung cells. As in other kinds of cancer, lung cancer cells grow and divide abnormally.
Each type of cancer is named according to the type of cell from which it originates. The origin of lung cancer is in the cells of the lung. And other cancers that spread to the lung are not lung cancer, for example, a liver cancer that has spread to the lung is still a liver cancer.
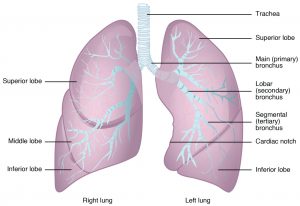
The lungs are the main organs of the respiratory system. Their function is to exchange the gases that enter and leave the body. Cells need oxygen to live, and this gas enters the lungs, whence it passes into the blood which carries oxygen to all cells of the body. And lungs also remove carbon dioxide (a gas produce by cells) from the blood. That is to say, through breathing, we inhale oxygen and expel carbon dioxide.
When we inhale, the air passes through the throat to the windpipe or trachea. Then, air enters the lungs through the bronchi, that branch into the lungs in smaller airways called bronchioli. At the end of each bronchiole there are bunches of alveoli wrapped in blood vessels. The exchange of gases in and out of the blood occurs here, in the alveoli.
The right lung has three lobes and the left lung two lobes. Lobes are delimited parts within the lung, and each one receives the air from a bronchus.
Lungs are covered by a tissue called pleura. It has two layers: the outer layer is called parietal pleura and the inner layer is called visceral pleura. The space between them is called the pleural cavity, which is filled with a small amount of liquid called pleural fluid. Sometimes, in lung cancer, some of the cancer cells can be in the pleural fluid.
Throughout our body, including the lungs, there is a clear fluid called lymph which gives cells food and water, and also contains immune cells to fight germs. Lymph is distributed by vessels, and it passes through small structures called lymph nodes. There are lymph nodes in the lung along the bronchi, and they are connected with others placed near the trachea and on the neck.
 The symptoms caused by lung cancer may be due to: 1) the tumour itself; 2) the tumour extension inside the chest; 3) the metastatic spread of the tumour, and 4) non-metastatic systemic manifestations (these are called paraneoplastic symptoms and can appear in any part of the body, for example, an increased body temperature).
The symptoms caused by lung cancer may be due to: 1) the tumour itself; 2) the tumour extension inside the chest; 3) the metastatic spread of the tumour, and 4) non-metastatic systemic manifestations (these are called paraneoplastic symptoms and can appear in any part of the body, for example, an increased body temperature).
Cough is the most frequent symptom. Other symptoms can be shortness of breath (dyspnoea), blood in sputum (haemoptysis), fever, fatigue or loss of weight.
When the tumour involves other tissues it could result in: bigger lymph nodes (for example, on the neck), shoulder and arm pain or chest pain (due to nerve involvement), difficulty in speaking or dysphonia (due to paralysis of a vocal cord), difficulty in swallowing (when the tumour compresses the oesophagus).
If the cancer spreads to another part of the body, symptoms and signs may appear in the affected systems, for example, neurological or bone symptoms.
But sometimes a lung nodule is found by chance in an imaging test in a person without symptoms or signs. In this case, it will be necessary to study the nodule to know whether it is a cancer or not.
Smoking tobacco is the biggest risk factor for lung cancer. The more a person smokes, the greater the risk of suffering from lung cancer. If a person stops smoking, the risk decreases. But the risk is higher in those who have been smokers than in those who have never smoked. And the risk of lung cancer is greater among people exposed to second-hand smoke than in people without any exposure to smoke.
Uranium — a substance found in rocks and soil — is a cancer-causing agent. Miners of uranium have a high risk of developing lung cancer. As uranium decays, a gas called radon is produced and gets into air and water, and it can accumulate in buildings, including homes. The risk of lung cancer depends on how much radon is in the home.
Other agents which can cause lung cancer are asbestos, arsenic, beryllium, cadmium, chromium, nickel, coal smoke, soot, silica and diesel fumes.
There are two lung diseases which can increase the risk of lung cancer: chronic obstructive pulmonary disease (COPD) and the widespread pulmonary fibrosis.
The risk of lung cancer is higher in smokers with a family history of smoking, especially when there are several cases in the family.
The risk of lung cancer may be increased in people with a smoking-related cancer (stomach, bladder, kidney, pancreatic, cervical, or head and neck cancers, or acute myeloid leukaemia) and in people who have had lymphoma.
 To reach the diagnosis of lung cancer and know the spread of the tumour, a series of tests will be necessary: medical history, physical exam, blood tests, computed tomography (CT) of the chest and upper abdomen, and biopsy.
To reach the diagnosis of lung cancer and know the spread of the tumour, a series of tests will be necessary: medical history, physical exam, blood tests, computed tomography (CT) of the chest and upper abdomen, and biopsy.
In some cases, treatment for smoking or additional tests can be necessary, for example, other imaging, lung functioning or biomarker tests.

The first thing the doctor does is to investigate the patient’s history or medical record. This includes questions to the patient about his/her health problems and treatments received during their life. Other questions are about the patient’s symptoms, and about medicines that the patient is taking now or has previously taken.
Doctors ask about symptoms that may be related to lung cancer, such as: cough, chest pain, difficulty in breathing, loss of weight and appetite , etc. To know these details is very important for doctors when staging the lung cancer.
Doctors also ask about the medical history of close blood relatives of the patient, because some cancers may exist in families. The members of the patient’s family who are important for medical history are parents, grandparents and siblings. And the age at which a relative had the disease is also important.
Doctors also ask about smoking: whether the patient smokes or has smoked in the past. The total amount smoked is calculated by packets per day and number of years of smoking.
 This is the study of the patient’s body, and its purpose is to look for signs of the disease. For example, in the examination the doctor hears the noise that the air makes when it goes in and out of the lungs. If there is an abnormal noise, this may be a sign of lung disease.
This is the study of the patient’s body, and its purpose is to look for signs of the disease. For example, in the examination the doctor hears the noise that the air makes when it goes in and out of the lungs. If there is an abnormal noise, this may be a sign of lung disease.
The physical exam includes the measurement of the temperature and weight of the body and the measurement of the pulse, blood pressure, and breathing rate. Doctors listen to the patient’s lungs, heart and gut, and also examine the nose, ears, mouth, eyes and skin. Another assessment is of performance: the patient’s ability to do daily activities, which is useful for knowing whether the patient can undergo certain treatments or not.
 The basic laboratory tests give a picture of the patient’s general health. They are usually: 1) Complete blood count (CBC), which measures parts of the blood, including red blood cells, white blood cells and platelets. The number of these cells can change in cancer and other diseases, and some treatments can also cause changes. 2) Biochemistry profile, which serves to know how the kidneys, liver, bone and other organs are working. Abnormal biochemical levels can be caused by the spread of cancer or by other health problems.
The basic laboratory tests give a picture of the patient’s general health. They are usually: 1) Complete blood count (CBC), which measures parts of the blood, including red blood cells, white blood cells and platelets. The number of these cells can change in cancer and other diseases, and some treatments can also cause changes. 2) Biochemistry profile, which serves to know how the kidneys, liver, bone and other organs are working. Abnormal biochemical levels can be caused by the spread of cancer or by other health problems.
There are other laboratory tests for testing biomarkers, usually on tissue samples. Biomarkers are molecules which can be in the tumour, and their presence or absence is used to plan treatment, since some treatments are only effective in tumours with a certain biomarker. Examples of biomarkers are mutations in the EGFR gene or rearrangements in the ALK gene.
Imaging refers to pictures of the inside of the body. It serves to see which parts of the body have cancer. It is performed and interpreted by radiologists. Some imaging uses contrast. This is a ‘dye’ that makes the picture clearer.
Sometimes a lung nodule is found by chance with imaging, and at other times when evaluating a patient with symptoms compatible with lung cancer. The tumour is visible in imaging: a computed tomography (CT) or a positron emission tomography (PET).
When CT and PET are used together it is called a PET/CT scan.
The characteristics of the lung nodule allow radiologists to know whether it can be a lung cancer.
For example, large nodules are more likely to be cancerous than small nodules. And the density of the nodule is important because it is usually related to the speed of growth of the tumour.
Imaging of the chest and upper abdomen serves to find the tumour and to know where to perform the biopsy, and also for identifying the stage of the cancer.
Additionally, there are some imaging tests to check whether there is metastasis of cancer outside the lung: 1) FDG PET/CT is performed with a radiotracer called fluorodeoxyglucose (FDG). This is a radioactive marker that accumulates at the points where cancer cells exist, and they can be seen with this technique. 2) Magnetic resonance imaging (MRI).

 To confirm the existence and know the type of lung cancer it is necessary to see the cells of the tumour by microscopy. These cells can be obtained by: 1) removing tissue samples, which is a biopsy, or 2) removing fluid samples, or aspirating cells with a needle, which is a cytology, because the sample is composed of cells more than tissue.
To confirm the existence and know the type of lung cancer it is necessary to see the cells of the tumour by microscopy. These cells can be obtained by: 1) removing tissue samples, which is a biopsy, or 2) removing fluid samples, or aspirating cells with a needle, which is a cytology, because the sample is composed of cells more than tissue.
Histopathological tests will be performed on the tumour and lymph nodes removed by surgery. And before this, in some cases there will be a biopsy using bronchoscopy, a procedure to see the inside of airways and take some samples. To analyse lymph nodes there is a procedure called mediastinoscopy, which allows surgeons to see and perform biopsy on lymph nodes between lungs, and the results of their histopathological tests are useful for staging lung cancer. Sometimes staging can be done with mediastinoscopy without bronchoscopy. And sometimes biopsy might not be done until the surgeon proceeds to remove the tumour.
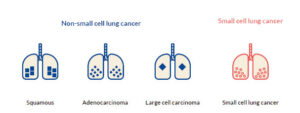
Lung carcinomas are divided into two groups based on how the cancer cells look by microscopy. This is called histologic typing:4,7
There are more types of NSCLC which are rare, for example, the adenosquamous carcinoma, the sarcomatoid carcinoma, etc.
Therapy of lung cancer depends on its histological type and stage, but also on the presence or absence of biomarkers and the physical state. Treatments include surgical resection and chemotherapy. In general, patients with early-stage lung cancer are treated by surgery, and patients with advanced or metastatic disease by chemotherapy. Radiotherapy is used in some cases.
If the patient is a smoker, he/she should stop smoking. This is very important, because smoking can limit how well the treatment works. But the stress of having a cancer may make it more difficult to give up smoking. Doctors advise how, and they help patients to stop smoking.
Once doctors have verified that a patient has a lung cancer, and once they know the stage, they will propose a plan of treatment. Primary treatment is the main treatment used to eliminate cancer, and it can be surgery, chemoradiation, radiation therapy or a combination of these.
Treatments for lung cancer can produce side effects.
Surgery
When possible, surgery is used as the primary treatment in NSCLC. Surgery is not used in SCLC (in this type of lung cancer other treatments are used).
The surgeon will remove the lung tumour and lymph nodes. The tumour will be removed with ‘surgical margin’, which means that the tumour is removed together with some normal-looking tissue round its edge. The pathologist, in the microscopical analysis, will check whether there are cancer cells in the surgical margin, and whether there are cancer cells in the lymph nodes.
Chemoradiotherapy
In some stages of NSCLC, when cancer grew or spread outside the lung, cancer chemoradiation is used instead of surgery. Chemoradiotherapy means having chemotherapy and radiotherapy treatment together. Chemotherapy uses drugs to destroy cancer cells. These drugs circulate throughout the body in the bloodstream. And radiotherapy uses radiation over the lung to destroy cancer cells8. This treatment may greatly reduce the extent of cancer. After this treatment, there is a standard treatment with durvalumab, which may control cancer for a longer period of time.
Chemotherapy
The most common chemotherapy drug is cisplatin, which is often combined with other chemotherapy drugs. Usually chemotherapy is administered before radiotherapy starts, as a drip into the patient’s arm every 3 to 4 weeks. It might continue during the radiotherapy treatment, or when radiotherapy ends. Chemoradiotherapy can cause side effects, such as tiredness, sickness, a sore throat, and a cough and breathlessness.
The treatment of the small-cell lung cancer (SCLC) is by chemotherapy and radiotherapy (no surgery), as long as they can cover the entire area affected (tumour and lymph node). In other cases, the treatment is chemotherapy. The most commonly used drugs are cisplatin and etoposide. Radiotherapy is administered at the same time. Due to the high frequency of brain metastasis, a prophylactic cranial irradiation is recommended.
Immunotherapy
Normally, immune systems recognise and fight cell cancers. But if the cancer appears, it is because the immune system has not worked properly to eliminate abnormal cells (cancer cells). Some immunomodulator drugs can help the immune system to recognise and fight cancer cells.
Some lung cancers produce particular proteins, such as PD-1 or PD-L1, which stop immune cells from recognising and destroying the cancer cells. There are immunomodulator drugs called checkpoint inhibitors which block these proteins. Once PD-1 or PD-L1 proteins are blocked, the patient’s immune cells can attack lung cancer cells. But checkpoint inhibitors do not work for all lung cancers, they only work for cancers with particular proteins.
Checkpoint inhibitors that have been approved by the EMA for some types of advanced lung cancer are atezolizumab, durvalumab, and pembrolizumab. (Another checkpoint inhibitor for lung cancer called nivolumab has been withdrawn at the request of the marketing authorisation holder). Several other checkpoint inhibitors are currently being tested in clinical trials for lung cancer.
consectetur adipisicing elit, sed do eiusmod tempor incididunt laboret dolore magna aliqua. Ut enim minim veniam quis nostrud exercitation ullamco laboris.
Website Under Construction
We are currently rebuilding our website, and look forward to its launch later in 2026.
Until then, this website is not being updated. Feel free to continue browsing, or visit our news site for the latest updates.